Cannabidiol (CBD) is a phytocannabinoid and present typically in low concentrations within the cannabis sativa flower. It is purported and investigated for its hypothesized and observed beneficial psychotropic and biological effects in various domains. With societal acceptance of cannabis consumption on the rise in the US, we are increasingly seeing CBD-focused products hit the open market and interest in these potential benefits on mind and body.
For some time, I was one who found benefit in CBD. Typical flower with its high concentrations of THC produced far too many adverse effects for me, but it was undeniable that I saw positive effects on stress and levels of depression. This was one of my go to coping aids for the longest time, and my responsibilities as an adult built throughout my career, I wanted a way to continue using cannabis products without the added anxiety, and diminished cognition of THC. I was able to find that in low THC, high CBD vapes that added terpenes back in to the mix.
This worked well for awhile, but as I entertained alternate ideas with the realisation that cannabis didn’t do enough for me, I became interested potential interactions. There’s always some potential that when trying new treatments that they will fail, so my intention wasn’t to make a seamless transition to something else. This is somewhat of a philisophical area of interest for me, experimenting on myself, and for various reasons, but suffice it to say, I feel it is important to know the ways in which the powerful substances we so often casually put into ourselves affect our biochemical makeup and the systems they form or act upon.
Cannabidiol is an inhibitor some P450 isoforms. These enzymes are present throughout cells but are concentrated highly in the liver. They serve to break down various compounds, endogenous or exogenous to the body, and play a critical role in metabolism. Notably, they process xenobiotics, eliminating foreign substances such as medicines and toxins alike. Inhibition of an enzyme results in reduction of its activity, and hence, reduced metabolism of the ligand(s) it binds with. This is one way that an interaction may occur between drugs, and is the focus of this writing.
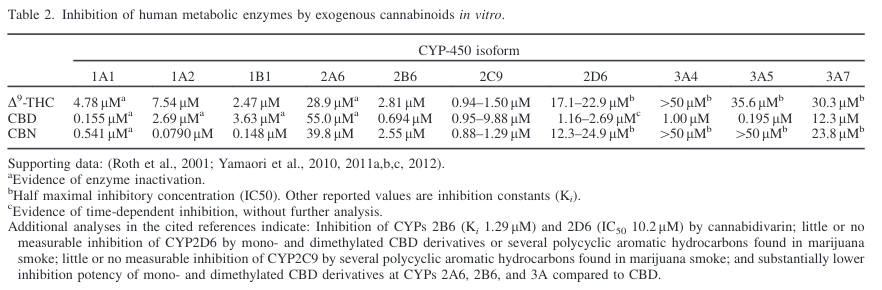
Let’s look at an in vitro study that produced some pharmacokinetic data on CBD:
CBD most potently inhibited CYP3A4 and CYP3A5 (IC(50)=11.7 and 1.65 μM, respectively). The IC(50) values of Δ(9)-THC and CBN for CYP3A4 and CYP3A5 were higher than 35 μM.
Fair bit of terminology here to understand. CYP is an abbreviation for Cythochrome P450. For example, CYP3A4 is one of the constellation of unique enzymes classified under it. I used the term isoform earlier, and you’ll see me use it throughout this analysis. An isoform is a categorization of proteins indicating similar functionally. IC50 is a measure of inhibition, and is the key data point in this quotation. It is a relative value, whose magnitude depends on the concentration of both substrate (the chemical undergoing reaction) and enzyme used in the assay.
This isn’t particularly helpful for me, as I have no idea at what concentration a given isoform is in my liver, and would be going off very rough population specific research. I’d prefer knowing the inhibitory constant, which is independent of enzyme concentration. This would tell me at what blood plasma concentration the substrate must be at to inhibit 50% of its action. There are exceptions, such as if it were the case that there is additional competition from multiple different substances for our isoform to bind with. That is another interaction point to consider. We know a decent amount of what a given isoform’s substrates are, though, and this can and should be cross-checked whenever considering taking a multiple significantly active substances. In any case, this inhibitory constant is called Ki, and we’ll have to look for it elsewhere for CBD.
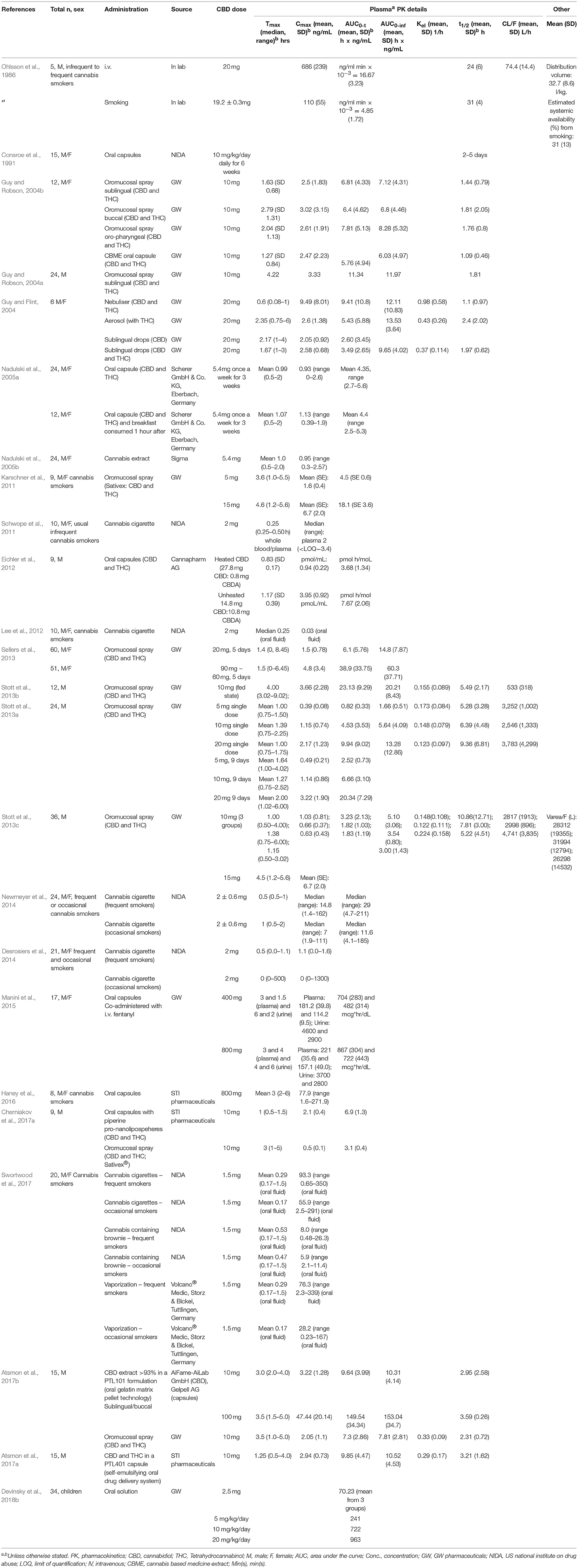
This meta-analysis will do. It has a nice table showing Ki values across a number of CYP isoforms (in vitro). Just what we wanted! Now, we need blood plasma concentration data. Check out this next table for differing routes of administration of CBD at specific doses.
{kind=link}
{kind=link}
In this table, we’re most interested in the value of Cmax. This is the maximum measured plasma concentration over the time span examined. I like this take for the sheer number of studies examined, but unfortunately, it doesn’t have much to say about the vaporization route, which is what I was primarily interested in. It lists one study that measured CBD in oral fluids after vaporization, but I’d prefer not to use this, as this isn’t the environment in which enzymatic reactions are primarily happening in, and concentrations are actually lower than that of blood plasma.
I did find one study to inform me on this ROA wherein 14 participants inhaled ~14 mg CBD along with THC in one group. No participants reported any use of medications, and passed drug tests on the morning of experimental sessions. The one downside if this study is that THC is a substrate of some isoforms in which CBD is an inhibitor of, which could be cause for confounding.
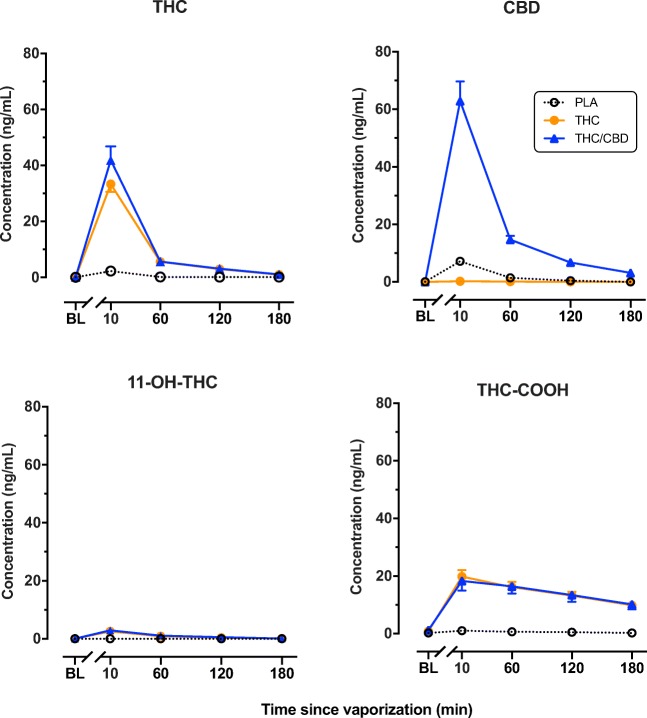
Here, we can see Cmax of CBD at around the 10 minute mark is around 60 ng/mL. Note the unit of measurement - nanomoles. The Ki values were mostly in micromoles. The closest we find to this figure is for CYP1A1 and CYP3A5, whose Ki values are 155 and 195 nM respectively. If we were investigating a drug which was metabolized by either of those isoforms, this may be cause for some concern and further research. But most drugs are metabolized by CYP2D6 and CYP3A4, whose Ki values are 1.16-2.69 and 1 uM. The Cmax of CBD reported is at least 17 times lesser than that required to produce significant inhibition there.
This is consistent with several meta-analyses’ claims:
Inhibitory constants and/or half maximal inhibitory concentration values of THC, CBD, and CBN at studied CYP-450 isoforms are generally well below the expected systemic concentrations of these cannabinoids with most use (Marinol U.S. prescribing information 6/2006; Sativex U.K. SPC 7/2012; Huestis, 2007; Johansson et al., 1987; Ohlsson et al.,1982, 1986) Further, regular dronabinol use or marijuana smoking had minimal impact on indinavir pharmacokinetic variables, suggesting a low clinical impact on CYP3A4 function (Kosel et al., 2002). Nonetheless, given the lack of inhibition data at several CYP-450 isoforms, the wide variability in cannabinoid product content and dosing, and the inherent imprecision of using concentration/inhibition potency ratios to predict in vivo drug interaction potential, clinically significant inhibitory effects cannot be ruled out entirely. Notably, the only studies found during this review that suggested clinically evident inhibition of CYP-450s in humans did not meet inclusion criteria, and suggested some possible weak CYP2C inhibition by CBD based on decreases in hexobarbital clearance and 11-hydroxylation of THC with concomitant CBD use (Benowitz et al., 1980; Nadulski et al., 2005).
I do wish I had found a study that have a higher sample size. They also didn’t provide raw data for each participant, or even a measure of standard deviation, so we can’t know if there are wild or just noteable variances from person to person. These limitations can’t give us high confidence that for most people, we’ll see roughly the same levels under the same conditions. We can do some inference based on similar levels demonstrated in the larger meta-analysis for other ROAs, and that does nudge up my confidence a moderate amount.
Sometimes, when considering experimental substance use, you have to make decisions with no or low quality data. My risk tolerance is calibrated such that this is enough for me to be comfortable with some drug combinations involving CBD. I knew approximately how much I was consuming on any given day, and it was pretty close to the concentrations studied. Had there been no data whatsoever, I were taking another medication that could produce dramatically different results with slight concentration difference, or I were consuming hundreds of milligrams of CBD, I would not be okay with this.
Research into phytocannabinoids is still young and rapidly developing. With growing popular support has came reformed general perception and regulation that has aided in produce interesting experimental outcomes. Yet, we still know relatively little about the specifics of many cannabis constituents pharmacodynamics. While this data may aid some in determining the potential of drug interaction, unknowns remain in which risk analysis becomes a matter of personal comfort and philosophy.
« Cautions against soy for folks on transfem HRT ✧ The odds of SARS2 infection »